Upon completion of this module the reader will be able to:
- Understand basic anatomy and functional anatomy for the ankle complex.
- Understand ankle sprain epidemiology
- Understand the mechanisms for the ankle sprains.
- Determine common risk factors that can lead to ankle sprains injuries.
Review the «Anatomy and Functional of the ankle joint» topic and the «Injury prevention strategies» topic first. Then read the “Anatomy of ankle joint”. Read the description of the “ Lateral Ankle Sprain injuries – Prevention strategies” and the corresponding presentation and then follow the proposed videos for some ideas of “ Lateral Ankle Sprain injuries prevention exercises”. End the session with the “Bibliography and the additional learning materials” and assess your understanding with the “Lateral Ankle Sprain injuries ” quiz.
Anatomy and function of the Anterior Talofibular ligament (ATFL)
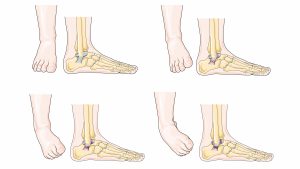
The Anterior Talofibular ligament (ATFL) is the most frequently injured of the lateral ligaments. The ATFL lies on the dorsolateral aspect of the foot, it starts from the lateral malleolus anteriorly and medially toward the talus at an angle of approximately 45° from the frontal plane. The ATFL prevents anterior displacement of the talus from the mortise and excessive inversion and internal rotation of the talus relative to the tibia. The strain in the ATFL increases as the ankle moves from dorsiflexion into plantar flexion.

By Injury map – edit Injury Map – Free Human Anatomy Images and Pictures. Retrieved on 2019-08-10., CC BY 4.0, https://commons.wikimedia.org/w/index.php?curid=69188254
Ankle injuries in wrestling – Prevention Strategies
Ankle
Ankle sprains include lateral ligament complex sprains, medial ligament complex sprains, and distal tibiofibular joint (‘‘high ankle’’) sprains (Kaplan et al., 2011; Lievers & Adamic, 2015).
Lateral ankle sprains are the most reported ankle ligamentous injury (Kaplan et al., 2011; Lievers & Adamic, 2015), Excessive inversion and internal rotation of the rearfoot, coupled with external rotation of the lower leg, results in strain to the lateral ankle ligaments. If the strain in any of the ligaments exceeds the tensile strength of the tissues, ligamentous damage occurs. Increased plantar flexion at initial contact appears to increase the likelihood of suffering a lateral ankle sprain. The anterior tibiofibular ligaments (ATFL) is the first ligament to be damaged during a lateral ankle sprain, followed most often by the calcaneofibular ligament (CFL) (Hetrel, 2002).
However, high ankle sprains typically result in the longest recovery periods, averaging 13.9 days compared with 8.1 and 10.7 days for lateral and medial ankle sprains, respectively (Lievers & Adamic, 2015; Waterman et al., 2011).
The distal tibiofibular (‘‘high ankle’’) joint is composed of the distal tibia and fibula and superior surface of the talus. The joint is supported by the anterior- and posterior-inferior tibiofibular ligaments, interosseous ligament, and interosseous membrane (Hermans et al., 2010; Williams et al., 2015). Sprains to this ligamentous complex most commonly occur from contact with another player that results in ankle dorsiflexion and foot external rotation (Markolf et al., 2013). This unique mechanism of injury and associated recommendations for a slow progressing rehabilitation (Markolf et al., 2013; Hunt et al., 2015) highlight the necessity to better understand the epidemiology and etiology of high ankle sprains to prevent and better rehabilitate these injuries.
NCAA Injury Surveillance Program high ankle sprain data and athlete-exposures (AEs) from 25 sports were evaluated. High ankle sprain injury rates per 10,000 AEs were calculated. The overall high ankle sprain injury rate was 1.00 per 10,000 AEs. Overall, 56.7% of high ankle sprain injuries occurred during competitions, and 9.8% of high ankle sprain injuries were recurrent. Men’s football (2.42/10,000 AEs), wrestling (2.11/10,000 AEs), and ice hockey (1.19/10,000 AEs) had the highest high ankle sprain injury rates. In sex-comparable sports, men had higher injury rates (RR, 1.77; 95% CI, 1.28-2.44). Player contact was the most common injury mechanism (60.4%), and 69.0% of injuries resulted in >1 day of participation restriction, with 47.1% resulting in >7 days of participation restriction and 15.8% resulting in > 21 days of participation restriction. High ankle sprains resulted in significant participation restriction time from sport participation.
In prospective studies, ankle injuries range from 3.2 to 9.7% of all wrestling injuries. Garrick (1975) described the results of the first year of the Seattle High School injury study. Ankle injuries were 6/105 (6% of wrestling injuries in that portion of the study). The most common ankle injury is the lateral ligament sprain, which most often occurs during takedowns.
Mechanisms of injury
Excessive inversion and internal rotation of the rearfoot, coupled with external rotation of the lower leg, results in strain to the lateral ankle ligaments. If the strain in any of the ligaments exceeds the tensile strength of the tissues, ligamentous damage occurs. Increased plantar flexion at initial contact appears to increase the likelihood of suffering a lateral ankle sprain. The ATFL is the first ligament to be damaged during a lateral ankle sprain, followed most often by the calcaneofibular ligament (CFL).