Upon completion of this module the reader will be able to:
- Understand basic anatomy and functional anatomy for the knee complex.
- Understand the lateral (LCL) and medial collateral ligament (MCL) injury epidemiology
- Understand the mechanisms for the LCL and MCL injuries.
- Determine common risk factors that can lead to the LCL and MCL injuries.
- Incorporate exercises as part of the prevention strategy for the LCL and MCL injuries.
Review the «Anatomy and Functional of the knee joint» topic and the «Injury prevention strategies» topic first. Then read the “Anatomy of LCL and PCL”. Read the description of the “ Lateral and Medial Collateral Ligament injuries in soccer – Prevention strategies” and the corresponding presentation and then follow the proposed videos for some ideas of “ LCL and MCL injury prevention exercises”. End the session with the “Bibliography and the additional learning materials” and assess your understanding with the “Lateral and Medial Collateral Ligament injuries in soccer” quiz.
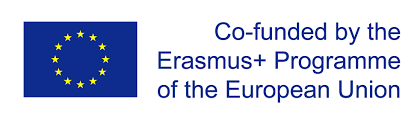
Lateral collateral ligament (LCL) is a cord-like ligament on the lateral side of your knee that forms part of the posterolateral corner. It originates from the lateral femoral epicondyle and attaches to the head of the fibula. MCL ligament is found on the inner aspect of the knee joint and is the largest structure situated on the medial side. The LCL stabilizes the lateral side of the knee joint, mainly in varus stress and posterolateral rotation of the tibia relative to the femur. The LCL acts as a secondary stabilizer to anterior and posterior tibial translation when the cruciate ligaments are torn. It is primary restraint to varus rotation from 0-30° of knee flexion. As the knee goes into flexion, the LCL loses its significance and influence as a varus-stabilizing structure. When the knee is extended, the LCL is stretched.
Figure 1: An illustration of knee joint
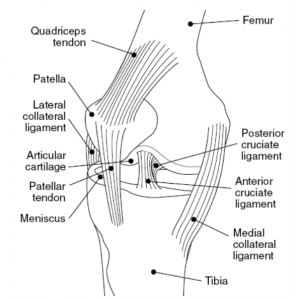
The medial collateral ligament is a primary static stabiliser of the knee and assists in passively stabilising the joint. The MCL also prevents an anterior movement of the tibia and hyperextension.
Figure 2: An illustration of knee joint
Τhe proposed preventive strategies for knee injuries include four phases and they propose specific preventive exercises :
Phase I : Muscular conditioning to restore dysfunctional movement patterns that can impede performance
1a. Inhibition: Inhibit through foam rolling the over-activate muscles: gastrocnemius & soleus, adductors, Tensor fasciae latae & Iliotibial band, and the short head of the biceps femoris.
1b.Muscle lengthen: Specific lengthening exercises with static or neuromuscular stretches for gastrocnemius & soleus, adductors, Tensor fasciae latae & IT-band, and the short head of the biceps femoris
Phase II: Muscular performance: Modifying strength and conditioning movements
Specific activation exercises through strengthening exercises or positional stabilization exercises for the anterior and posterior tibialis, gluteus medius, and gluteus maximus. Core strength.
Phase III: Functional exercise: Building efficient movement patterns
Starting with proper athletic position, always warm up before playing, perform different Squats and Walking Lunges. Do balance, agility-changing direction and jumping and landing exercises.
Lateral Collateral ligament (LCL) and Medial Collateral ligament (MCL) injuries in soccer – Prevention Strategies
Injury epidemiology
Injuries to the lateral and medial collateral ligaments are common in the general population, but the MCL injuries occur more often than the LCL injuries. The MCL and the anterior cruciate ligament (ACL) are the most commonly sprained knee ligaments. In soccer, MCL injuries are even more common and they occur in conjunction with other knee injuries. The MCL is injured in at least 42% of knee ligament injuries, with isolated MCL injuries accounting for 29% of ligamentous knee injuries alone. Females, especially younger ones, are at an increased risk to sustain a MCL injury
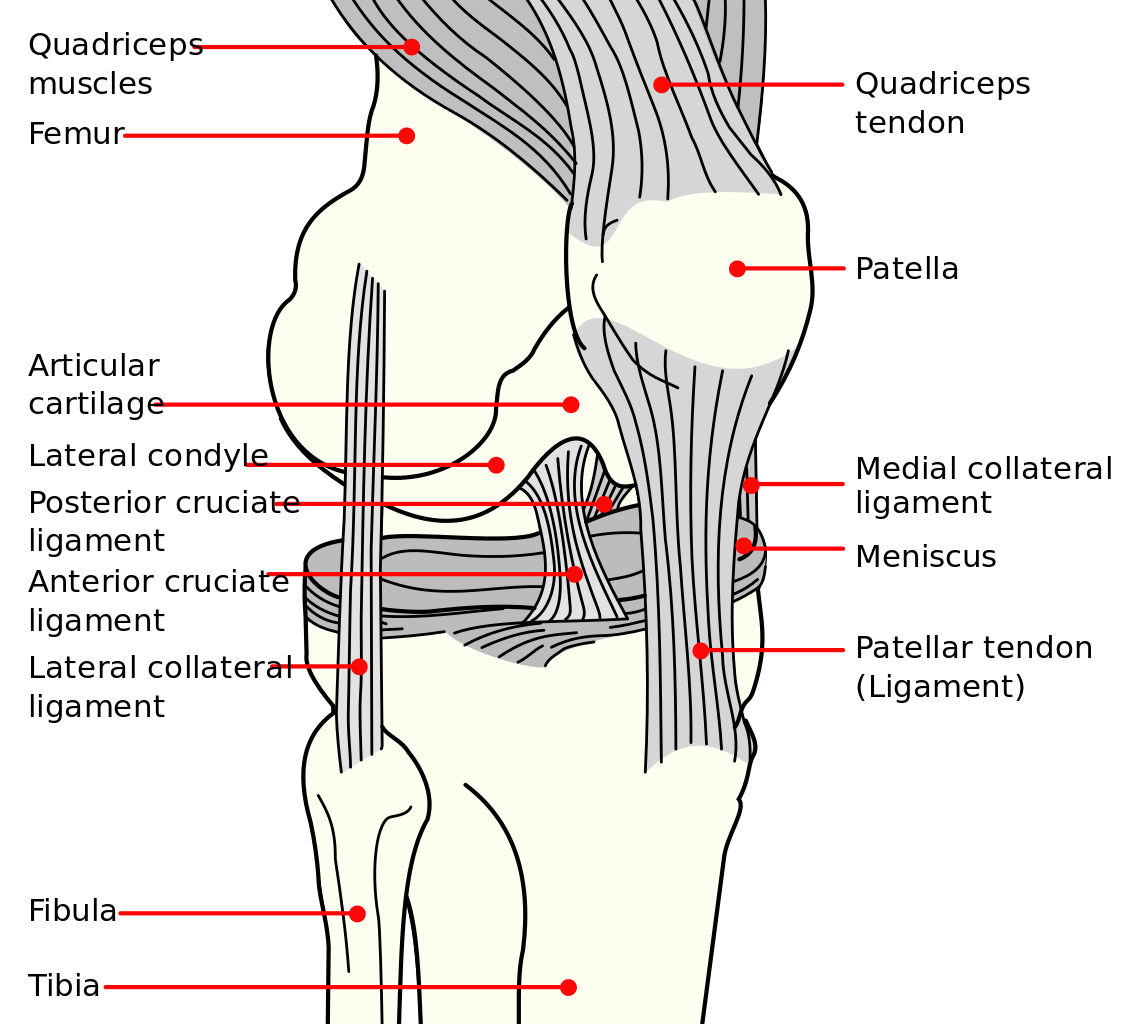
Mechanisms of injury
Illustration of injury of anterior cruciate and medial collateral ligament. By OpenStax College – Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013., CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=30131679
A MCL injury is a stretch, partial tear, or complete tear of the ligament on the inside of the knee. This ligament is injured from a valgus force on the knee and it is frequently combined with an ACL injury. Although the LCL is less commonly injured than the MCL, injuries of this ligament may be more disabling because these structures are subjected to greater forces when we walk. During walking, when the foot contacts the ground the physiological varus angulation of the limb axis increases and reaches maximum and the LCL is stretched. Common injury mechanisms include increases in varus loading of the knee, lateral rotation of the tibia when the foot is locked on the ground (weight-bearing) or loss of ligamentous elasticity due to repeated loading.