Upon completion of this module the reader will be able to:
- Understand basic anatomy and functional anatomy for the lower limbs complex.
- Understand the knee Injury epidemiology
- Understand the mechanisms for the ankle and knee injuries.
- Determine common risk factors that can lead to the ankle and knee injuries.
- Incorporate exercises in order apply a prevention strategy for the ankle and knee injuries Meniscus injuries.
- Review the «Anatomy and Functional of the knee joint» topic and the «Injury prevention strategies». Read the description of the “Lower limb Prevention strategies” and the corresponding presentation and then follow the proposed videos for some ideas of “Lower limb prevention exercises”. End the session with the “Bibliography and the additional learning materials” and assess your understanding with the “Lower limb injuries”
The soft tissue structure in the knee includes 2 menisci, the MM (located on the inside of the knee) and LM (located on the outside of the knee). These crescent-shaped pads of fibrocartilage rest on the tibial condyles and form a concave surface for the femoral condyles to rest on.
These cover approximately 2/3 of the tibia surface and are thicker on the outside and thinner on the inside appearing triangular in cross section. They fill the space between the leg bones and cushion the femur so it doesn’t slide off or rub against the tibia. The menisci play a very important role in the proper working of the knee. Essentially, they serve as cushions to decrease the stress caused by weight bearing and forces on the knees.
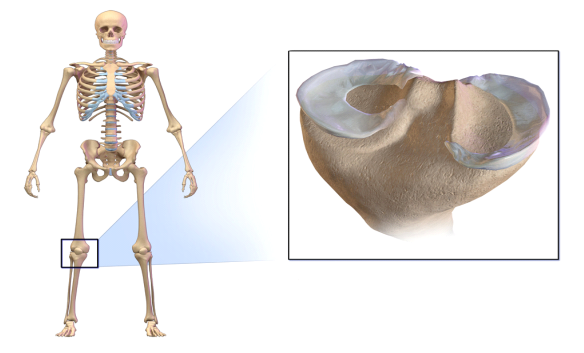
By Andrewmeyerson – Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=49411618
Figure: An illustration of knee joint and the menisci. The menisci are “thin discs” that lie between the thigh (upper leg) and the tibia (lower leg)
They work like shock absorbers, supporting the load by compressing and spreading the weight evenly within the knee. The menisci assist with the proper movement (arthrokinematic) of the femur and tibia during flexion and extension. They help stabilize the knees when in motion, reduce friction within the joint, and lubricate and protect the articular cartilage surrounding the tips of the bones from damage due to wear and tear.
Knee
The lower extremity is classically the most commonly injured area in wrestling with more number of injuries occurring at the knee followed by the ankle (Strauss & Lanese, 1982; Pasque & Hewett, 2000). These injuries are usually season ending and often require surgical intervention.
Knee injuries are more common in college wrestlers, not only in frequency, but also in severity. Knee injuries are the most common injury responsible for missing 3 weeks or more of college wrestling and the most common site of injury requiring surgery (Yard et al., 2008).
In Agarwal & Mann (2016) study more number of knee injuries occurred in attack position. This can possibly be attributed to poor technique. More number of knee injuries i.e. 93.33%, were sustained in competitions while only 4.49% injuries occurred during practice in Agarwal & Mann (2016) study (incidence density ratio = 20.7). In Agarwal & Mann (2016) study 60.56% knee injuries occurred in the age group of 20 – 24 years, while 29.57% injuries were seen in the age group of 15 – 19 years. Out of total knee injuries, 61.97% injuries occurred in wrestlers practicing for 5 – 10 years, while 35.21% occurred in wrestlers practicing for 0 – 5 years. Use of legs in FS and hands and arms in GR as per rules possibly makes these wrestlers more vulnerable to lower and upper extremity injuries, respectively.
In Agarwal & Mann (2016) study 83.09% injuries occurred in FS wrestlers while 16.90% occurred in GR wrestlers. The proportion of injuries i.e. total knee injuries in wrestlers practicing FS wrestling was also more (IPR = 1.39). A study by Wroble et al. (1986) revealed that there were 11.5 knee injuries per 100 wrestlers per year requiring a week or greater time loss. Pasque & Hewett, (2000) found that the mean total time lost from injury was 5 days (range, 1 – 39days). There were 18.11 knee injuries per 100 wrestlers per year requiring a week or greater time loss in our study.
In prospective studies, knee injuries have ranged from 7.6 to 44% of all wrestling injuries (Strauss & Lanese, 1982; Hewett et al., 2005). In the only study with the percentage of knee injuries below 10%, Lorish et al. (1992) described injuries in tournaments to wrestlers aged 6 – 16 years. The knee injuries, in Agarwal & Mann (2016) study also were quite high comprising 37.7% of all injuries reported. These injuries tend to be severe. Over an 11 year period in NCAA wrestling, 65% of injuries requiring surgery involved the knee. In the same study, 21% of injuries leading to greater than one week absence from competition involved the knee (Jarret et al., 1998). Barroso et al. (2011) in their study found that the highest number of lesions involved the knee (25.5%), followed by the shoulder (20%) (Barroso et al., 2011). However, more number of injuries occurred to the shoulder (24%) followed by the knee (17%) in a study by Pasque & Hewett, (2000).
According to Wroble et al. (1986) wrestlers with previous knee injuries were at high risk for re-injury. Kordi et al. (2012) reported that 77% of all injuries were acute ones (new injuries), 10% of injuries were recurrent, 2% of injuries were unresolved injury from the preceding year and 1% of them were due to a recent worsening of an unresolved injury. In Agarwal & Mann (2016) study 71.83% of the knee injuries were new injuries while, 28.16% were recurrent. The most common knee injuries are sprains, which constitute 30 – 65% of all knee injuries.
Prepatellar bursitis is a very common type of knee injury, and is fairly unique to wrestling (Strauss & Lanese, 1982; Mysnyk et al., 1986). Mysnyk et al. (1986) documented 28 cases of prepatellar bursitis, representing 21% of all knee injuries.
Meniscus
The soft tissue structure in the knee includes 2 menisci, the MM (located on the inside of the knee) and LM (located on the outside of the knee). These crescent-shaped pads of fibrocartilage rest on the tibial condyles and form a concave surface for the femoral condyles to rest on. These cover approximately 2/3 of the tibia surface and are thicker on the outside and thinner on the inside appearing triangular in cross section. They fill the space between the leg bones and cushion the femur so it doesn’t slide off or rub against the tibia. The menisci play a very important role in the proper working of the knee. Essentially, they serve as cushions to decrease the stress caused by weight bearing and forces on the knees. They work like shock absorbers, supporting the load by compressing and spreading the weight evenly within the knee. The menisci assist with the proper movement (arthrokinematic) of the femur and tibia during flexion and extension. They help stabilize the knees when in motion, reduce friction within the joint, and lubricate and protect the articular cartilage surrounding the tips of the bones from damage due to wear and tear.
Meniscal injuries are also common, with a relatively high proportion of lateral to medial meniscus tears (Hewett et al., 2005). Lateral meniscus injuries represented 46% of the total number of meniscal injuries in a study and there were 45% lateral versus medial meniscectomy in a study on 56 meniscectomies in wrestlers (Strauss & Lanese, 1982; Baker et al., 1985). Lateral meniscus injuries were 58.3% of all meniscal injuries in Agarwal & Mann (2016) study.
ACL
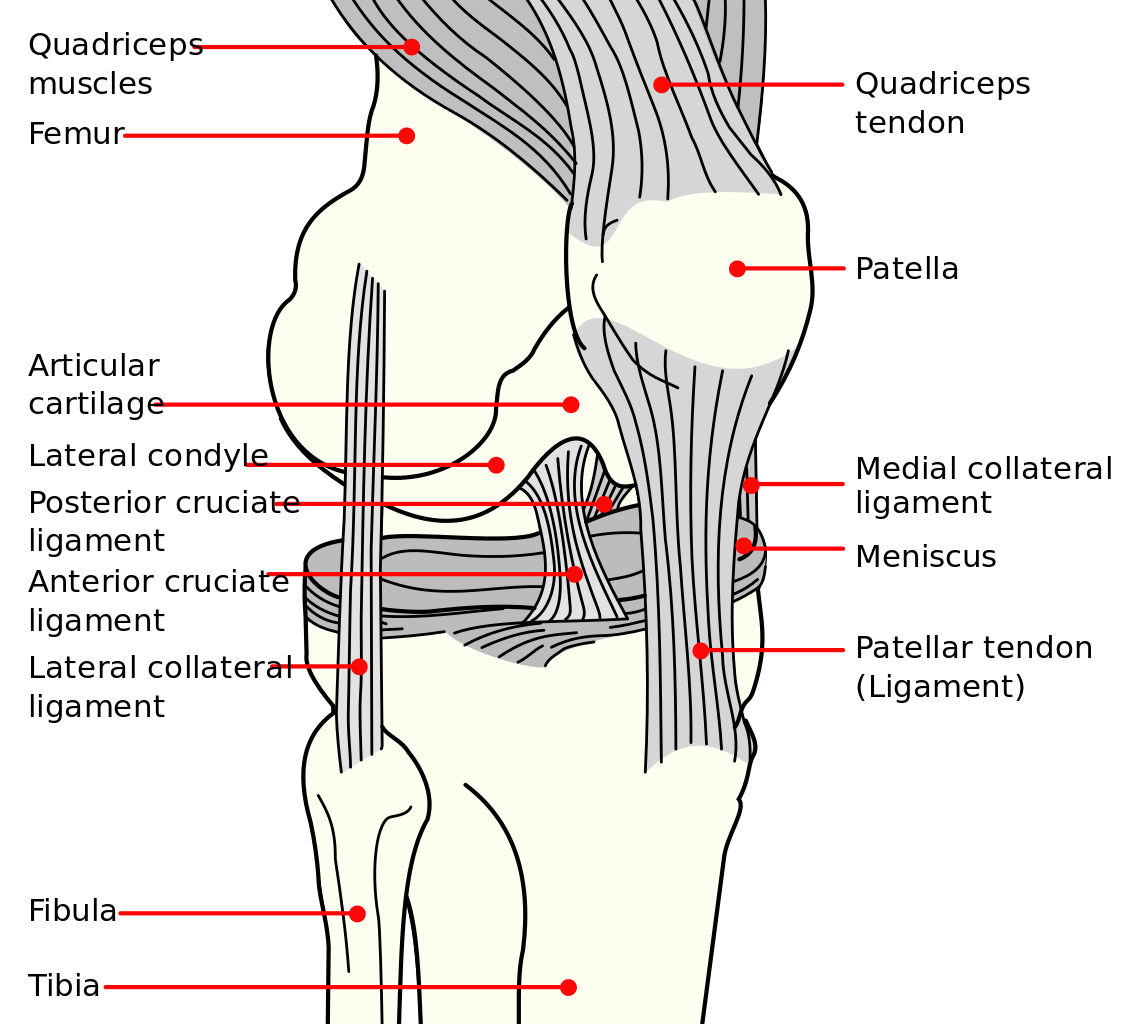
The ACL originates from the medial and anterior aspect of the tibial plateau and runs superiorly, laterally, and posteriorly toward its insertion on the lateral femoral condyle. The ACL is composed of the anteriomedial and posteriolateral bundles. Together, these bundles provide approximately 85% of total restraining force of anterior translation. It also prevents excessive tibial medial and lateral rotation, as well as varus and valgus stresses. To a lesser degree, the ACL checks extension and hyperextension. Together with the posterior cruciate ligament (PCL), the ACL guides the instantaneous center of rotation of the knee, therefore controlling joint kinematics.
Anterior cruciate ligament (ACL) ruptures are among the most commonly studied injuries in orthopaedic research. The incidence of ACL ruptures is estimated to range from 30 to 78 per 100,000 person-years. After ACL reconstruction, 61% to 89% of athletes successfully return to sports, typically at 8 to 18 months after reconstruction, depending on the level of play.
Anterior cruciate ligament tears were noted in 14 of 256 knee injuries in one study (Strauss & Lanese, 1982). Similarly, three of the 64 knee injuries were ACL tears in a study by Wroble et al. (1986). In Agarwal & Mann (2016) study 8/77 injuries were ACL tears.
MCL
The medial collateral ligament (MCL) of the knee is the major stabilizer against valgus force and is frequently placed under great stress in the sport of wrestling (Kiningham & Monseau, 2015).
MCL injuries are relatively common in young athletes. Most injuries occur with direct contact, placing a valgus force on the knee, or from cutting maneuvers with the foot planted, creating a valgus moment in the knee. The addition of a rotational force may injure the posterior oblique ligament as well as the MCL (Indelicato, 1995). The 3-layer concept of the anatomy of the medial knee described by Warren and Marshall (1979) notes that after the superficial sartorial fascial layer, the middle layer contains the superficial MCL and posterior oblique ligament, and the deep layer contains the true capsule of the knee joint and the deep MCL.
Usually, MCL injuries are graded based on the American Medical Association’s classification according to the medial knee opening with valgus stress placed with the knee in 30° of flexion. Grade 1 opens <5 mm, grade 2 opens between 5 and 10 mm, and grade 3 opens >10 mm (American Medical Association, 1966). The vast majority of MCL injuries are treated nonoperatively with emphasis on early rehabilitation, range of motion exercises, and weightbearing when pain free (Miyamoto, et al., 2009). Despite the lack of surgical management, these common injuries can cause significant lost time to return to sport or activity.
The overall IR of MCL injuries in a young athletic cohort was 7.27 per 1000 person-years. Male intercollegiate athletes were over 2.6 times more likely to sustain an MCL injury than female intercollegiate athletes (Roach et al., 2014). The intercollegiate sports of wrestling, judo, hockey, and women’s rugby had the highest IRs of MCL injuries. There were 73% grade 1 MCL injuries, while 27% were grade 2 or 3. The average amount of time lost per injury was 23.2 days, with greater time lost with higher grade sprains than grade 1 sprains (Roach, et al., 2014).